
Case Study: Patient presents with a headache...

Patient presents with a headache – can you guess where their headache is coming from?
28 year old female presented to Jannali Physiotherapy & Sports Injury Clinic with a 1 week history of headaches.
I asked her if she was experiencing any neck pain – she replied yes, describing her neck (cervical) pain equal on both sides intermittently radiating into her mid back (thoracic). After further questioning she informed me that her headaches were constant, straight across her forehead – a ‘pressure’ feeling. She occasionally experiences dizziness and 3 days ago randomly felt nauseous, however when she laid down, this seemed to ease her nausea and headaches.
It’s always important to ask about every patient’s social life (e.g - what they do for work, how long is a typical day at work, how physically active they’re, how have they been sleeping, is there anything in their life that’s making them feel more stressed than usual right now and any beliefs around why they think they’re experiencing those symptoms). After questioning, these are some points that stood out to me as a physio:
She is an office worker. During COVID lockdown, she has been working from home. Her set-up is an office desk and chair (which she seems to think is ‘ergonomically’ a correct set up).
Normally tries to go to the gym 3-5x per week, but due to COVID isn’t. She is trying to go for a walk 3-4x per week now.
She notices that after long periods of sitting or towards the end of the day her headaches worsen. She also mentioned work has been quite busy lately and her work hours have increased, this has caused her a bit of stress recently.
She believes her headaches posturally related but unsure why or how because she say’s she constantly ‘thinks’ and tries to ‘correct’ her posture.
When a patient presents with a primary complaint of headaches, it’s extremely important that they’re screen for other different diagnosis and potentially more sinister pathologies. I excluded any sinister pathologies or differential diagnosis such as (but not limited to) jaw pain and vestibular impairments. There was no other significant health concerns.
When I voiced to the patient that their headaches might be coming from their neck, they had no idea that that could happen!
Before examining her neck I asked her to change 3 things for me:
More regular movement breaks at work
Walk every day
MOVE MORE
Your best position is your next position!
This patient was used to travelling to work (2 hours a day), walking to the station, having regular meetings throughout the day, working on her sit to stand desk at work and then going to the gym in the afternoons. Now all of a sudden, her physical activity has almost reduced by half (incidental and purposeful movement) and she is replacing this time with sitting for longer. I told her to think about her accumulative time she spends sitting a day and work on reducing it where she can.
I began assessing their neck (cervical spine). On examination, I found:
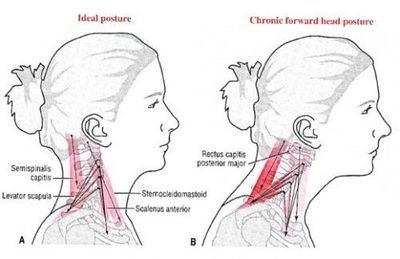
She had a forward head posture (her ears were about 5cm in front of her shoulder). We generally try to encourage that people work towards keeping their ears over their shoulders)
Her chin pocked forward of her forward. We generally try to encourage people to work towards keeping their chin in line with their forehead.
Her mid back (thoracic) was quite rounded and she struggled to extend back. Her shoulders were positioned down (depressed)
I showed this to her in a photo. I then asked her to modify this position to where she thought was correct. She was able to stick her chest out so she wasn’t so rounded through her mid back. Unfortunately, that was the only thing she changed. She was not aware of the position of her neck or her shoulders. I corrected this immediately using cues like ‘lengthen the back of your neck’ and ‘bring your head back onto an imaginary wall’.
I also told her to ensure that the height of her desk wasn’t too low so as to drag her shoulders down. She said she thought it was and I instructed her to raise the height of her desk.
I told her that muscle’s don’t like working in lengthened positions for too long. In fact, they don’t like being in any position for too long (good or bad). And if her shoulders are depressed it may be pulling on her neck muscles, which in term can be contributing to her headaches.
Her neck (cervical ROM) was slightly restricted when she looked up. I told her I wasn’t surprised because she most likely spends the majority of her day looking forward.
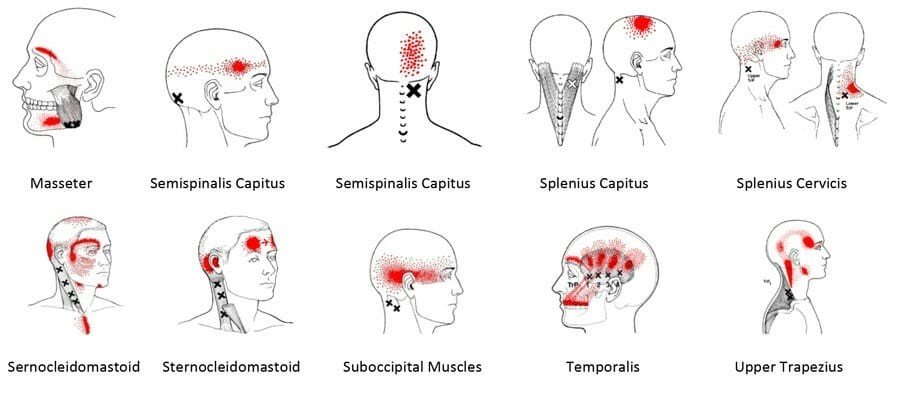
When I felt her neck she was extremely stiff on what we call C1, C2, C3 and C7/T1 segments. I explained to her that often, the first few segments of the upper neck play a big role in reproducing headaches due to the complex system of nerves around that area that also bring sensation to the face and head area. Humans, unfortunately perceive this sensation as a headache!
